
From Principle to Practice
What Patient Engagement Now Means and Why It Matters to People Living with Chronic Pain

In September 2025, the NIH Engaging the Public as Partners in Clinical Research (ENGAGE) Working Group released its draft report — a roadmap NIH has now formally accepted for how clinical research should partner with patients and communities. Early in the report is a single sentence that, if taken seriously, would change the way most research gets done:
“Clinical research engagement occurs when people, groups of individuals, communities, and/or organizations partner with researchers to plan, design, and conduct research so that the research and its outcomes are meaningful, actionable, or support understanding of disease for those who could benefit from the research.”
Read that again, slowly.
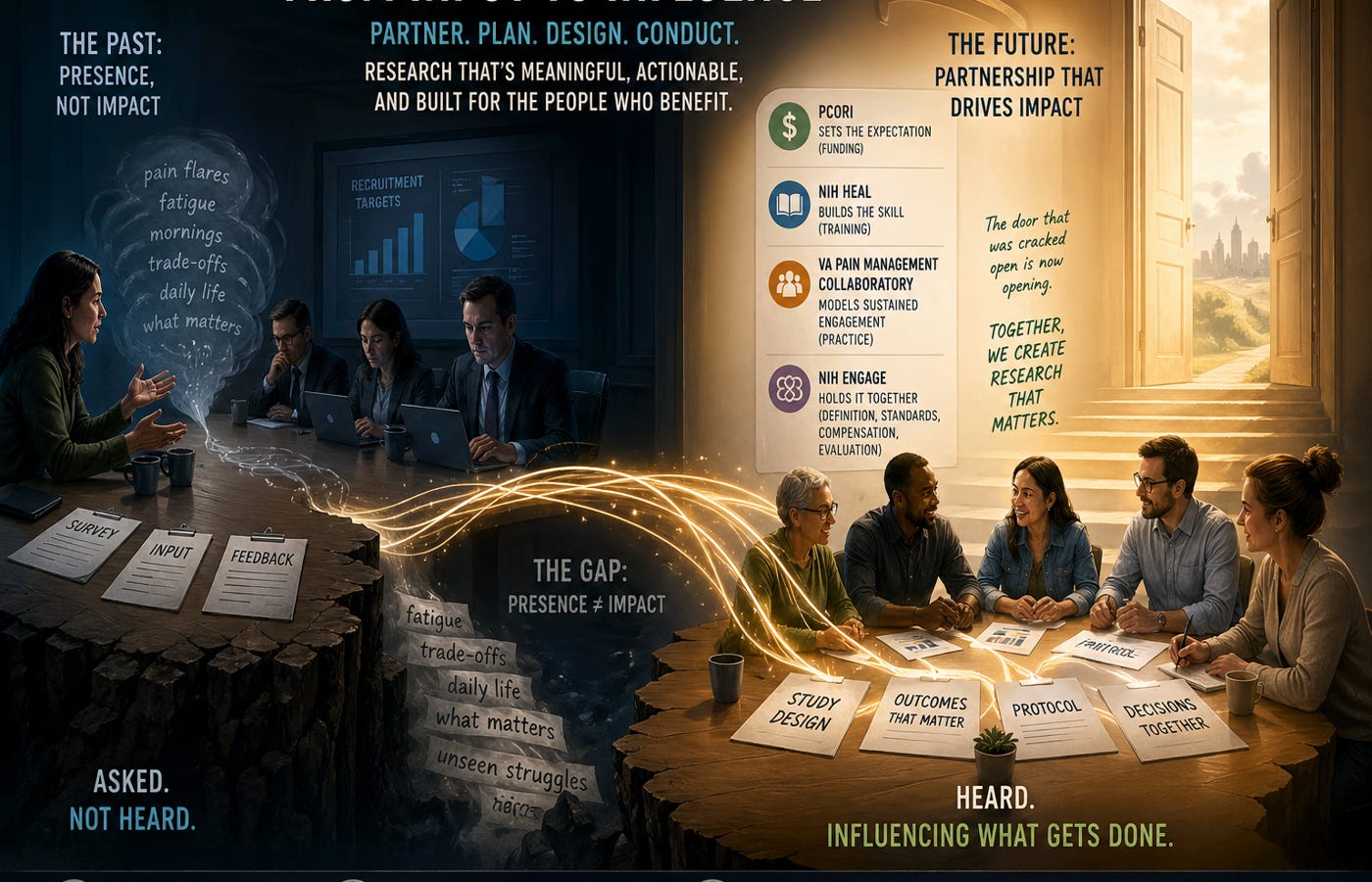
Partner.
Plan, design, and conduct.
Meaningful and actionable for the people who would benefit.
That’s a long way from being asked for feedback on a recruitment flyer. It’s the difference between input and influence. It’s also a long way from where a lot of research currently sits.
Most of us know the feeling.
You sit on a panel, fill out the survey, join the call. You answer the questions carefully. You describe what living with pain is like — the mornings, the trade-offs, the things that don’t show up in a clinic visit. And then, months later, you read the study, or the guideline, or the press release, and almost none of what you said is in it.
That gap — between being asked and being heard — is the part of patient engagement that doesn’t get talked about enough. We’ve solved for presence. We haven’t solved for impact.
For years, the conversation has been about whether people with lived experience should be at the table. We won that argument a long time ago. The question now is harder: when we are at the table, does anything we say change what gets done?
That gap shows up everywhere. It shows up in treatments that don’t fit real lives. It shows up in guidelines that miss the day-to-day reality of living with pain. It shows up in studies that measure what is easy instead of what matters.
And it matters now because something is finally shifting.
What’s Changing
What’s changing now is not one program or initiative, but a coordinated shift across how research is funded, taught, and carried out. You can see it clearly when you look across four efforts that, together, are redefining what engagement means in practice.
Patient-Centered Outcomes Research Institute is making engagement a condition of funding. If a research team wants the money, they must show how people with lived experience are built into the work, not consulted at the end, but integrated from the start. That’s a real lever because it changes incentives. Influence here isn’t a favor; it is tied directly to whether the work gets funded.
The NIH HEAL Initiative is focused on teaching researchers how to do this well. “Engage patients meaningfully” is not a skill most investigators were trained in, and HEAL is working to close that gap, especially for early-career researchers who will shape how this is done going forward.
The VA Pain Management Collaboratory has gone further than almost anyone by treating engagement as a sustained relationship. Their Patient Resource Group is not a one-study advisory board. It is a standing group of veterans who contribute across projects, over time. This is what engagement looks like when it is built into the infrastructure, not added on.
And then there is the report from the National Institutes of Health Engaging the Public as Partners in Clinical Research (ENGAGE) Working Group, the source of the definition above. NIH asked the Novel and Exceptional Technology and Research Advisory Committee to form the ENGAGE Working Group, co-chaired in part by Christin Veasley of the Chronic Pain Research Alliance, alongside experts from patient advocacy, community organizations, and clinical research. Their charge was to give NIH a unified vision for engagement. The resulting roadmap was formally accepted by NIH Director Dr. Bhattacharya, with implementation beginning in 2026.
Where PCORI sets the expectation, HEAL builds the skill, and the VA shows what sustained engagement looks like, ENGAGE holds it together. It defines what engagement is, names it as bidirectional, and, crucially, calls for equitable compensation and for monitoring and evaluating engagement so it cannot remain symbolic. That is where the field has been weakest and where ENGAGE does its most important work.
Taken together, these efforts tell a consistent story. Expectations are being set. Skills are being built. Real models exist. A common language is taking hold. The door that used to be cracked open is now opening in a way that is harder to ignore.
The Gap Nobody is Naming
Here is the part that doesn’t get said out loud: the expectations are moving faster than the system can keep up.
Researchers are now being told to engage patients meaningfully, but many of them have never done it before. Funders are demanding evidence of influence, but the tools to measure influence are still being built. People with lived experience are being invited into rooms where the role hasn’t been clearly defined, the support isn’t always there, and the respect isn’t always automatic.
That gap has a cost, and people with lived experience are usually the ones who pay it. We’re the ones who show up to a meeting and realize halfway through that we’re decoration. We’re the ones who give honest feedback and watch it disappear into a report we never see. We’re the ones who do unpaid emotional labor explaining our lives to people who treat the explanation as data extraction. Compensation, when it exists, is often nominal. The expectation that we’ll show up, share, and represent entire communities is rarely matched by the structures that would make that work sustainable.
It’s also worth saying plainly: the people most likely to be invited into these rooms are often the most articulate, the most networked, the ones who can take unpaid time to attend. The chronic pain community includes many people who can’t. Any honest conversation about engagement must keep asking who isn’t in the room.
What This Asks of Us
If engagement is going to mean influence — and that’s the whole point — then those of us with lived experience must step into the role differently than we have before.
That doesn’t mean becoming researchers. It means becoming partners, which is its own thing. Partners ask how their input will be used. Partners expect to be in the decisions, not just the discussions. Partners notice when engagement is performative and say so. Partners learn enough about how research works to push back when something doesn’t fit real life.
This is uncomfortable work. It asks people who are already managing a chronic condition to also manage a learning curve, navigate institutional dynamics, and sometimes be the person who says the hard thing in a room full of credentials. It is not fair that this falls to us. It also might be the only way the change sticks.
Where Support Groups Come In
Community matters more in this moment than most people realize.
Support groups are usually described as places where people come for understanding, for coping strategies, for the simple relief of being with others who get it. All of that is true. But something else happens in those rooms that has, until now, been largely invisible to the research world.
People learn how to talk about their experience.
They figure out which words capture the fatigue that doesn’t show up on a pain scale. They hear someone else describe a trade-off they’ve been making for years without realizing it had a name. They watch a newer member struggle to articulate something, and they help her find the language. Over months and years, people in support groups develop something that looks a lot like fluency in their own lived experience.
That fluency is exactly what research engagement now requires.
Which means support groups are quietly doing something larger than support. They’re preparing people to step into roles where their voices can shape what gets studied, how it gets studied, and what counts as a meaningful outcome. That isn’t the original purpose of these communities, and it shouldn’t replace it. But it’s a real thing that’s happening, and it’s worth naming.
For those of us who facilitate or lead these groups, that opens up a few choices. We can keep the discussion entirely inward, which is a legitimate and important function. Or we can also, when the moment is right, invite the bigger conversation in: what would you want a researcher to know? What outcome would actually matter to you? Has anyone here ever been part of a study, and what was that like?
When that conversation starts happening in community spaces, something shifts. The insight that used to stay in the support group starts traveling. And the research that used to happen at a distance starts coming back in a form people can use.
To the Researchers Reading This
If you’re a researcher or funder reading this, the ask is straightforward and aligns with what ENGAGE itself recommends. Bring people with lived experience in early, before the protocol is written. Pay them properly. Define their role clearly enough that they know whether they’re being consulted or shaping decisions. Close the loop — tell them what you did with their input, including when you didn’t use it, and why. And keep asking who isn’t in your engagement structure, because the easiest patient advisors to recruit are rarely the ones whose lives are hardest.
What I’m Watching For
I’ll know engagement has really changed when a few things are true.
When study questions start sounding like the questions people actually ask each other in support groups. When outcomes include the things that wreck a day — fatigue, sleep, the cost of doing one good thing and paying for it for three days afterward — alongside the pain scores. When findings come back to the community in plain language, fast enough to be useful. When people with lived experience are co-authors and co-investigators, not just acknowledgments. When compensation is real, not symbolic. When “engagement” stops being a section in a grant application and becomes the way the work is done.
ENGAGE’s definition gives us something to hold the system to.
“Meaningful, actionable, or support understanding of disease for those who could benefit from the research.”
That’s the standard now. It’s in writing. It’s been formally accepted. The work ahead is making sure it doesn’t become another sentence everyone agrees with and nobody enforces.
We aren’t there yet. But the direction is right, and the institutions are moving. What happens next depends on whether enough of us — researchers, funders, facilitators, and people living with pain — step through the door together, and whether we’re honest with each other about what we find on the other side.
Reference: Engaging the Public as Partners in Clinical Research (ENGAGE) Working Group. Draft Report. Novel and Exceptional Technology and Research Advisory Committee (NExTRAC), National Institutes of Health. September 2025.
Disclaimer: The views, positions, and recommendations expressed in this article are based on my personal experiences and independent research. They are solely my own and do not necessarily reflect the views, policies, or positions of the American Chronic Pain Association (ACPA).
Acknowledgment: The original draft of this article was edited with the assistance of AI.
Brilliant context, thank you Tom. Especially your emplasizing that we as chronic pain sufferers are partners with researchers. I would hope that is an essential aspect of how most studies get better findings with we our inputs.
I will now reframe my narrative with providers that we are "partners" forming a solutions together to lessen our ongoing pain challenges. Much appreciated. Molly.
Brilliant, Tom.